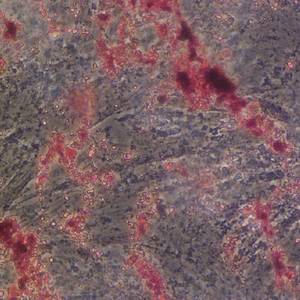
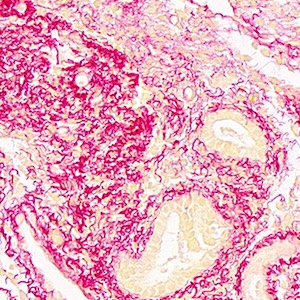
Detection of non-papillary, non-invasive transitional cell G1 carcinoma as revealed by increased DNA instability and other cancer markers
Published: 29 June 2009
Abstract Views: 634
PDF: 362
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
Downloads
Download data is not yet available.
Publication Facts
Metric
This article
Other articles
Peer reviewers
0
2.4
Reviewer profiles N/A
Author statements
Author statements
This article
Other articles
Data availability
N/A
16%
External funding
N/A
32%
Competing interests
N/A
11%
Metric
This journal
Other journals
Articles accepted
57%
33%
Days to publication
0
145
- Editor & editorial board
- profiles
- Academic society
- N/A
- Publisher
- PAGEPress Publications, Pavia, Italy

To learn about these publication facts, click ![]()
PF is maintained by the Public Knowledge Project
Citations




How to Cite
Hirose, M., Sun, A., Okubo, T., Noriki, S., Imamura, Y., & Fukuda, M. (2009). Detection of non-papillary, non-invasive transitional cell G1 carcinoma as revealed by increased DNA instability and other cancer markers. European Journal of Histochemistry, 49(2), 199–210. https://doi.org/10.4081/944
PAGEPress has chosen to apply the Creative Commons Attribution NonCommercial 4.0 International License (CC BY-NC 4.0) to all manuscripts to be published.